
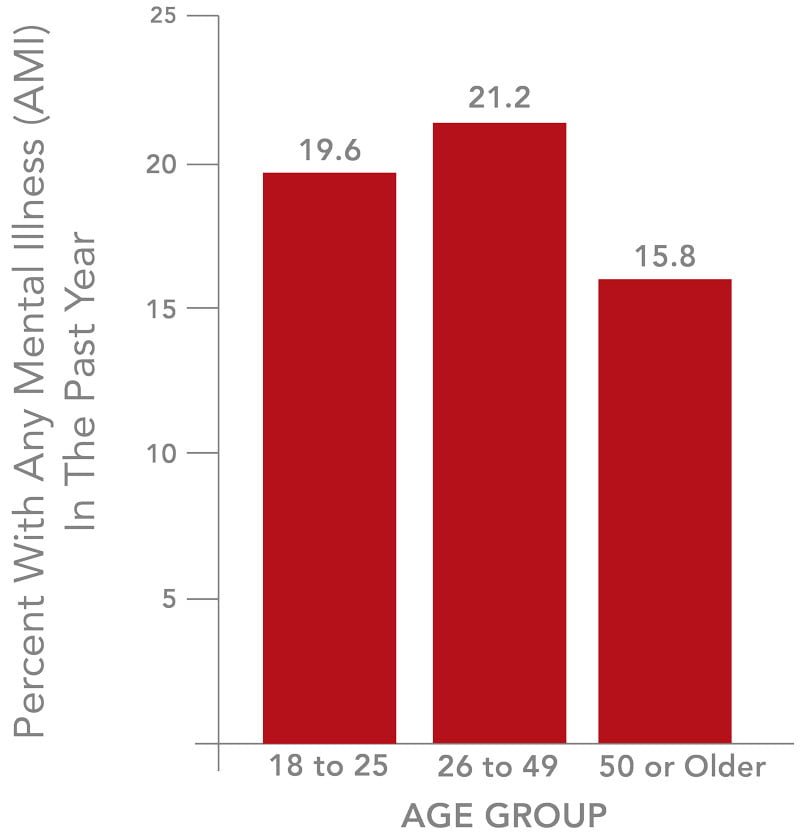
In the United States, It is estimated that 18.6% of the population currently suffers from at least one type of mental illness.1 With greater numbers of people gaining the means and motivation to access treatment for their conditions, the current supply of behavioral health providers and facilities is falling short of demand. Additionally, as care has evolved and become more efficient, often outmoded facilities are hard-pressed to deliver the best, most cost-effective care. This document seeks to outline the trends and best practices to create environments that meet these challenges.
It is estimated that 18.6% of the population currently suffers from at least one type of mental illness.
Beyond the pervasive rates of mental illness in the population, healthcare reform is enabling greater numbers of people to access care. According to the Centers for Medicare & Medicaid Services, 50% of Medicaid enrollees have a mental health diagnosis. With an expected 62 million people gaining insurance coverage, demand will reach a tipping point.1 Many communities already struggle with capacity to provide care and a large number of patients are crowding emergency rooms where they are treated for mental illness less effectively and at a greater expense.
Mental illness has also proven to make the overall cost of a person’s healthcare much more expensive. Substance Abuse and Mental Health Services Administration (SAMHSA) data from its National Survey on Drug Use and Health (NSDUH) – 2013 indicates people with mental illness are more likely to have chronic health conditions such as high blood pressure, asthma, diabetes, heart disease, and stroke than those without mental illness. For those with diabetes, the cost of treating this health condition is as much as four times higher when a co-occurring condition such as depression or alcohol addiction is untreated.1 Mental illness prevention, early detection, and effective treatment are key in lowering the overall cost of healthcare, so much so that special provisions have been written into the Affordable Care Act to facilitate access to behavioral health services.
While current capacity is struggling to meet demand for treatment, behavioral health services have greatly improved and evolved over time. Advanced medications and the deinstitutionalization of mental healthcare have played the most significant part in improvements over the past several decades. The sterile institutions of yesteryear no doubt played a large part in the negative stigma surrounding mental illness. Luckily, today’s facilities have advanced greatly to provide individualized care in a more comforting environment. The emphasis has now been placed on recovery, rather than confining patients. Branding for organizations and facilities in recent years reflects this shift, with the preferred terminology being “behavioral health” or sometimes not even referencing services, rather than referring to “mental illness” or stigmatized terms such as “insane.”
It has become widely accepted among providers and architects that the design of healthcare facilities can affect patient outcomes. In recent years, a number of academic studies have focused on the relationship between specific building design elements and positive outcomes for patients. Using these findings, architects can take an evidence-based approach to building behavioral health facilities and thus support patients’ psychological and physical needs.
The Department of Veterans Affairs3 is recognized as a top authority on behavioral services. They recommend the following principles to provide the most effective care:
Principle #1
Mental health services should be recovery-oriented
Principle #2
Mental health services should be provided in a therapeutically enriching environment
Principle #3
Mental health services should be provided in a safe and secure environment
Principle #4
Mental health services should be integrated and coordinated
Principle #5
Mental health services should be provided in settings that respect and can accommodate a diverse range of populations and care needs
With this background in mind, some current trends in design can be described to create an effective care center. First, by bringing services directly to the patient, therapeutic opportunities can be maximized. Combining inpatient and outpatient treatment into one pavilion allows for the combining of staff expertise. Closer proximity allows for staff knowledge sharing, as well as patient tracking from inpatient to outpatient care, which can help achieve the goal of improving and driving down the cost of population health. Patients themselves experience the improvement and are more secure when services are inside their units, including physical activity spaces and pharmacy services. Outpatients can also attend all of their appointments in one location and with fewer visits.
One of the most notable facility trends is the creation of non-institutional, homelike care spaces through various efforts including effective use of color, fabrics, and furnishings. Artwork and customization of lights and alarms can help support this effort. While balancing patient safety is of the highest priority, it has been found that homelike environments can decrease patient aggression, support recovery, induce shorter stays, and allow patients to participate in their treatment.7
Another design element evidenced to reach these same goals is the use of private patient rooms and even private bathrooms. These rooms obviously address the desire for patient privacy, but beyond that have been found to improve patient engagement in care and lessen withdrawal when compared to rooms accommodating multiple patients.7
When shifting focus to the larger inpatient unit, flexible census units allow for rooms to be transitioned between different treatment services to accommodate fluctuating patient censuses. Examples are the creation of additional space for geropsychiatric (elder) care or segregation between genders. This also allows care to be more cost-effective because the provider is not overcommitting their resources for one service in an integrated facility if the census falls.
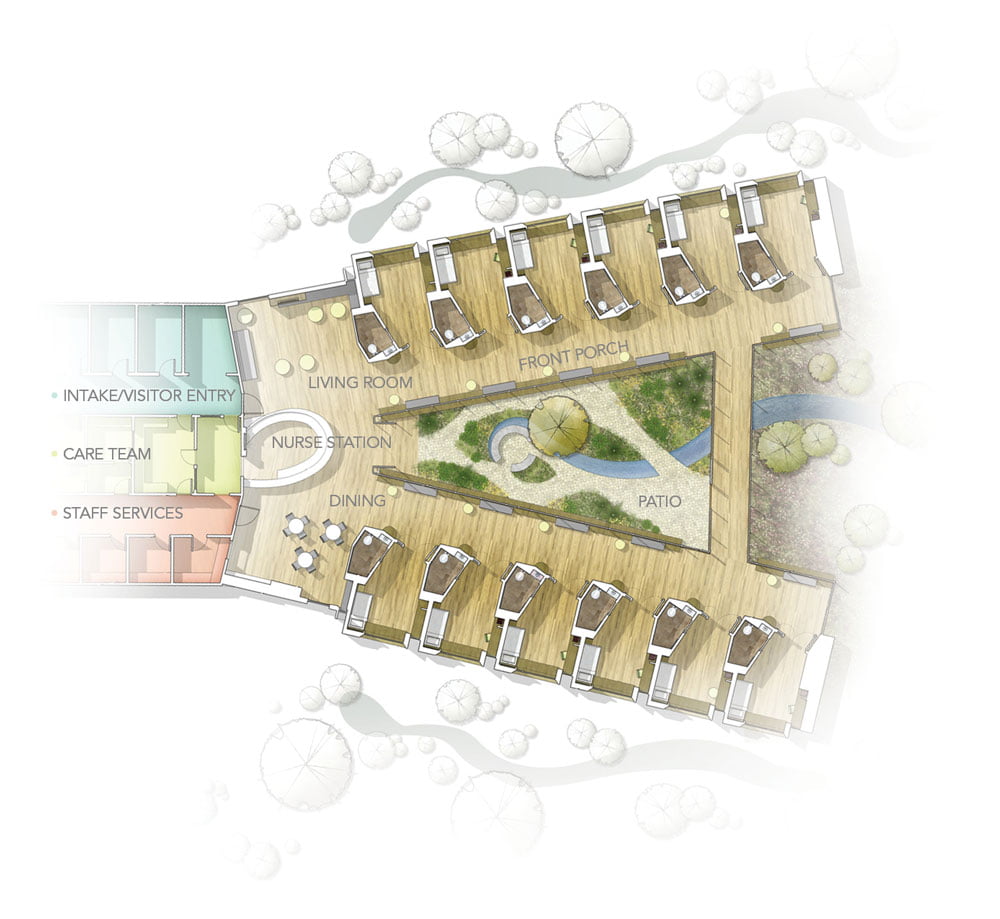
In addition to flexible beds, units can be designed with a neighborhood concept in mind. This helps create a more homelike environment, with groups of patients sharing activity and dining spaces, and often participating in therapy together. Providing the majority of services in one “household” or “neighborhood” allows care to be normalized and for patients to feel more participatory in their treatment, which can shorten stays and improve outcomes.
In both inpatient and outpatient treatment areas, onstage and offstage design is becoming a prevalent way to improve care. Inspired by the Disney concept of front stage areas for park visitors and backstage areas for staff, this concept involves the use of private staff corridors and work areas, while treatment areas and corridors are primarily used by patients. Though a relatively new concept, onstage-offstage design has been shown to improve patient and staff satisfaction while also reinforcing the idea of a homelike environment.4 Further, it can improve safety and security by lessening disruptions for patients and creating retreats for staff in the case of an emergency.
Units designed with a neighborhood concept in mind helps create a more homelike environment, with groups of patients sharing activity and dining spaces, and often participating in therapy together.

One final trend that should be accounted for is the design of technology-enabled spaces. The Centers for Medicare and Medicaid Services and other groups have advocated for increased use and funding of technology in behavioral healthcare, including incentivizing meaningful use of electronic medical records (EMRs). The Behavioral Health IT (BHIT) Coalition has stated:
“To appropriately care for patients with severe mental illness and co-morbidities, they assert, there must be tight care coordination and communication between the behavioral health provider, primary care provider and medical specialists to keep the patient from cycling in and out of intensive care. Behavioral health providers are as critical, if not more so, to a ‘healthy exchange’ and ‘safety network’ as any of the other organizations receiving funding.”2

Within specific episodes of treatment, technology-enabled spaces improve communication between staff and with patients about their treatment. Additionally, they allow for improved patient observation and security.
Meeting current and future demand for behavioral health treatment benefits the community at large. Not only are issues able to be addressed and improve overall health and prosperity, but the cost of delivering healthcare can be better controlled when patients are not crowding emergency rooms and are receiving better monitoring and more efficient care. Up-to-date, flexible ambulatory and behavioral facilities can serve surrounding communities as models for population health and a patient-centered design model in the continuum of care.
- Substance Abuse and Mental Health Services Administration. (2013). “Results from the 2012 national survey on drug use and health: Summary of national findings.” NSDUH Series H-46, HHS Publication No.(SMA) 13-4795. Substance Abuse and Mental Health Services Administration, Rockville, MD. http://archive.samhsa.gov/data/NSDUH/2k12MH_FindingsandDetTables/2K12MHF/NSDUHmhfr2012.htm.
- Billings, E. (2015). “Behavioral health acutely needs EHRs.” Healthcare IT News. http://www.healthcareitnews.com/blog/behavioral-health-acutely-needs-ehrs.
- Department of Veterans Affairs, Veterans Health Administration. (2008). “Uniform mental health services in VA Medical Centers and Clinics.” Washington, DC: VHA Handbook 1160.1. http://www.mirecc.va.gov/VISN16/docs/UMHS_Handbook_1160.pdf.
- Edmonds, J. (2013). “Research briefings: Emerging exam room types and provider perceptions.” ERDMAN.
- Levin, A. (2007). “Psychiatric hospital design reflects treatment trends.” Psychiatric News, 42(2), 9.
- National Institute of Mental Health. http://www.nimh.nih.gov/health/statistics/index.shtml.
- Ulrich, R., Bogren, L., & Lundin, S. (2012). “Toward a design for reducing aggression in psychiatric facilities.” In Arch 12: Architecture/Research/Care/Health. Chalmers, Gothenberg.


